Study 6: pre-examine the AR experience
Together with Janel Bosscha (Master of Media Innovation student at BUas) we went into a search adventure on why and how to make use of augmented reality to create a cue exposure treatment for AUD based on the VRET RECOVRY.
WHY: Theory shows many advantages of using AR (compared to VR) in CET, such as personalization of the environment (integration in natural environment), visibility of own body, transportable and easy / natural to use (comfortable), affordable, control and safety. However, it also has some potential drawbacks such as privacy issues, lower level of (technical) realism (small fov) and rendering power. Moreover, although previous studies showed promising results for ARET, these were all based on anxiety based on phobia and fear (claustrophobia, animal phobia and fear of speaking) or different conditions (ADHD and social anxiety) and different addictions (mainly related to smoking). Hence, it remains unclear how to create an ARET for AUD treatment and the effects it can generate (compared to VRET), on experience, craving and recovery (reducing craving, increasing confidence, practice resistance, and reducing relapse).
WHAT: in this study we wanted to obtain more knowledge in the arguments, tresholds and recommendations in how to implement AR (RECOVRY) in Cue Exposure Therapy for AUD treatment on a technological, medical, and personal level. In addition to obtain more insights in the potential of adding more realistic (volumetric captured) digital humans in VRET and ARET. The insights are used to improve RECOVRY as a VRET tool as well as to create the first ARET aimed at AUD treatment
HOW: we interviewed twelve participants. Before the interviews RECOVRY was explained with the use of PowerPoint. During the interviews, RECOVRY VR and Augmented Reality examples, that included volumetric captured avatars (based on THRIVE, a medical training project), were demonstrated through the Nreal Light AR glasses together with the OnePlus 8T smartphone. During the interviews, we observed how the clients interacted with the AR technology. Measures: implementation strategies AUD treatment phases and expected benefits and tresholds (ethics) for patients (medical experts), technological possibilities now and in future (AR versus VR) and Volumetric Capturing possibilities and benefits compared to low level avatars in treatment (technological experts). Concerning the ex-clients we measured: usability AR tecnology, evaluation, recommendation, realism experience, and recommendations (concerning environments, cues, situations and elements that would evoke cravings).
WHO: four technological experts (either AR or Volumetric Capturing specialists from companies like 4dviews and 4dr studios), three medical experts (familiar with AUD and VRET treatment: therapist, psychotherapist and psychiatrist), and five DSM-V ex-clients participated in the study (sober between 2-5 years, three female).
WHEN & WHERE: the interviews took place at BUas (clients) and online or at the workppace for the specialists between June-August 2022.
RESULTS: participants mentioned many craving cues that also emerged in previous studies. These related to sounds (e.g., sounds of glasses, good music, background pub sounds), objects (glasses, ash trays, food, bottles and to personalize them with brands), environments (especially bar and home) and emotional contexts. These emotional contexts were negative (stress, home alone, sadness) or positive (fun with parents, friends and strangers), observed behavior (smoking, eating, drinking) and peer pressure (invitation to drink). Some mentioned the combination of positive and negative: “I started drinking as I felt lonely, but my relapse came from one drink offered at me at New Year's Eve”.
Moment of treatment: all experts agreed ARET treatment should be after detoxification. Although treatment often does not take place in a chronological order. ME1: “You can start whenever the detoxification has been completed’. Then they see a step approach for the future: (1) first in clinic with psychiatrist, (2) then at home with presence of psychiatrist and (3) finally they can try it at home alone. The clients either agreed or stated that home alone felt too risky. Other environments were not explicitly addressed in the interviews but popped up: “it [craving] really can come out of nowhere. So, in that sense, I also wonder, if I was going on vacation or away from home for other purposes, I would like to take such glasses [recovry] with me”. Many studies showed the importance of context that causes craving, especially in worlds like at home, kitchen, bar / pub, restaurant, party, supermarket, park and other public spaces. Some of these environments are challenging to implement in ARET treatment, such as a pub or restaurant, due to lack of control, safety and privacy issues. However, environments such as a kitchen, a park, walking pass a bar or supermarket, or at home seem doable and relevant.
Avatars: the tech experts stated that it would be very doable to add two volcap avatars in AR using the phone. Using more would reduce the quality. In addition, these avatars can interact (like shake hands) and eye contact, morphing and looping could further increase realism. The clients graded the volcap avatars as very high on realism, stated that realism does increase craving and expected that the craving would increase in the invitation to drink compared to the low-level avatars used in the VRET RECOVRY. “When I look through the phone, I am pretty sure I am in the real world. I feel like with the glasses, I will be in a situation that I will be really triggered”. Next step would be personalization of the avatars. Most participants did not like the idea of intoxicated avatars as that leads to aversion.
Invitation to drink: everyone agreed this causes craving and that his can be done in the same way in VR as in AR. Suggestions for improvements were to add personalization through names used in the voice. Although the preset in answer options works, some also suggested to have and ''open answer possibility': “Because
then you have the primary response instead of thinking first, like, ‘Well, just give me wine', because that is maybe less bad than if I say jenever”. Based on the situations described also other ideas for invitations were found: “A difficulty for me is whenever people look at me like I am weird whenever I say that I don’t drink any more. They are always like ‘you can only grab one, right?’. I also feel like people kind of push me out because I don’t drink”.
ARET: the particpants stated that compared to the VRET, the ARET feels less immersive, despite high realism in the avatars. On the one hand due to the technology (still in development), on the other hand as the field of view is small. However, the ARET was seen as highly Interesting as it can provide context and interaction in your own personalized world.
WHY: Theory shows many advantages of using AR (compared to VR) in CET, such as personalization of the environment (integration in natural environment), visibility of own body, transportable and easy / natural to use (comfortable), affordable, control and safety. However, it also has some potential drawbacks such as privacy issues, lower level of (technical) realism (small fov) and rendering power. Moreover, although previous studies showed promising results for ARET, these were all based on anxiety based on phobia and fear (claustrophobia, animal phobia and fear of speaking) or different conditions (ADHD and social anxiety) and different addictions (mainly related to smoking). Hence, it remains unclear how to create an ARET for AUD treatment and the effects it can generate (compared to VRET), on experience, craving and recovery (reducing craving, increasing confidence, practice resistance, and reducing relapse).
WHAT: in this study we wanted to obtain more knowledge in the arguments, tresholds and recommendations in how to implement AR (RECOVRY) in Cue Exposure Therapy for AUD treatment on a technological, medical, and personal level. In addition to obtain more insights in the potential of adding more realistic (volumetric captured) digital humans in VRET and ARET. The insights are used to improve RECOVRY as a VRET tool as well as to create the first ARET aimed at AUD treatment
HOW: we interviewed twelve participants. Before the interviews RECOVRY was explained with the use of PowerPoint. During the interviews, RECOVRY VR and Augmented Reality examples, that included volumetric captured avatars (based on THRIVE, a medical training project), were demonstrated through the Nreal Light AR glasses together with the OnePlus 8T smartphone. During the interviews, we observed how the clients interacted with the AR technology. Measures: implementation strategies AUD treatment phases and expected benefits and tresholds (ethics) for patients (medical experts), technological possibilities now and in future (AR versus VR) and Volumetric Capturing possibilities and benefits compared to low level avatars in treatment (technological experts). Concerning the ex-clients we measured: usability AR tecnology, evaluation, recommendation, realism experience, and recommendations (concerning environments, cues, situations and elements that would evoke cravings).
WHO: four technological experts (either AR or Volumetric Capturing specialists from companies like 4dviews and 4dr studios), three medical experts (familiar with AUD and VRET treatment: therapist, psychotherapist and psychiatrist), and five DSM-V ex-clients participated in the study (sober between 2-5 years, three female).
WHEN & WHERE: the interviews took place at BUas (clients) and online or at the workppace for the specialists between June-August 2022.
RESULTS: participants mentioned many craving cues that also emerged in previous studies. These related to sounds (e.g., sounds of glasses, good music, background pub sounds), objects (glasses, ash trays, food, bottles and to personalize them with brands), environments (especially bar and home) and emotional contexts. These emotional contexts were negative (stress, home alone, sadness) or positive (fun with parents, friends and strangers), observed behavior (smoking, eating, drinking) and peer pressure (invitation to drink). Some mentioned the combination of positive and negative: “I started drinking as I felt lonely, but my relapse came from one drink offered at me at New Year's Eve”.
Moment of treatment: all experts agreed ARET treatment should be after detoxification. Although treatment often does not take place in a chronological order. ME1: “You can start whenever the detoxification has been completed’. Then they see a step approach for the future: (1) first in clinic with psychiatrist, (2) then at home with presence of psychiatrist and (3) finally they can try it at home alone. The clients either agreed or stated that home alone felt too risky. Other environments were not explicitly addressed in the interviews but popped up: “it [craving] really can come out of nowhere. So, in that sense, I also wonder, if I was going on vacation or away from home for other purposes, I would like to take such glasses [recovry] with me”. Many studies showed the importance of context that causes craving, especially in worlds like at home, kitchen, bar / pub, restaurant, party, supermarket, park and other public spaces. Some of these environments are challenging to implement in ARET treatment, such as a pub or restaurant, due to lack of control, safety and privacy issues. However, environments such as a kitchen, a park, walking pass a bar or supermarket, or at home seem doable and relevant.
Avatars: the tech experts stated that it would be very doable to add two volcap avatars in AR using the phone. Using more would reduce the quality. In addition, these avatars can interact (like shake hands) and eye contact, morphing and looping could further increase realism. The clients graded the volcap avatars as very high on realism, stated that realism does increase craving and expected that the craving would increase in the invitation to drink compared to the low-level avatars used in the VRET RECOVRY. “When I look through the phone, I am pretty sure I am in the real world. I feel like with the glasses, I will be in a situation that I will be really triggered”. Next step would be personalization of the avatars. Most participants did not like the idea of intoxicated avatars as that leads to aversion.
Invitation to drink: everyone agreed this causes craving and that his can be done in the same way in VR as in AR. Suggestions for improvements were to add personalization through names used in the voice. Although the preset in answer options works, some also suggested to have and ''open answer possibility': “Because
then you have the primary response instead of thinking first, like, ‘Well, just give me wine', because that is maybe less bad than if I say jenever”. Based on the situations described also other ideas for invitations were found: “A difficulty for me is whenever people look at me like I am weird whenever I say that I don’t drink any more. They are always like ‘you can only grab one, right?’. I also feel like people kind of push me out because I don’t drink”.
ARET: the particpants stated that compared to the VRET, the ARET feels less immersive, despite high realism in the avatars. On the one hand due to the technology (still in development), on the other hand as the field of view is small. However, the ARET was seen as highly Interesting as it can provide context and interaction in your own personalized world.
STUDY 5: THE EFFECT OF AVATARS

Together with Laura Lasonna, student at the Master of Media Innovation (BUas), we investigated how recovered alcoholics experience digital humans’ implementation in the context of Virtual Reality Exposure Therapy for alcohol use disorder, and how they react to a drink invitation in Virtual Reality.
WHY: The feasibility study (see Study 3) revealed the desire of clients for a more realistic experience, that can be achieved by adding virtual humans to the virtual environment. Also, previous research shows ann increase in craving when digital humans are added, however that this also depends on the type of drinker, the type of interaction, the level of realism of the avatars as well as the visibility of other cues (e.g., alcohol presence). In addition, the use of CG avatars in 360 VR environments have never been studied. As such, it remains unclear what degree of visual fidelity is needed to stimulate an emotional response in simulated social interaction in the context of Cue Exposure Therapy for AUD, and how the presence of avatars affects the perceived realism of the exposure session and the craving levels of those individuals suffering from AUD. Hence, RECOVRY was updated with avatars to create social pressure by means of a virtual invitation to drink and we examined how low-fidelity avatars are experienced (level of realism) and the reasons behind how they (not) influence craving during the therapy.
WHAT: for this study RECOVRY 2.0 was developed in which we first transported and updated RECOVRY for the Oculus Quest 2 glasses (instead of Samsung VR), developed and implemented avatars in the RECOVRY 360 and CG worlds that represented the bar and the Livingroom. The avatars were avatars with a low level of realism, to reduce costs and prioritize the idea of creating many avatars and contexts (effectiveness). In addition, a call to action was created where the avatars offer a drink to the user and the user needs to select from a menu, using the Oculus Quest 2 controllers, that contains for options (a) yes, a beer, (b) yes, a wine, (c) yes, something stronger or (d) yes, but something without alcohol. This invitation to drink was offered by a male bartender in the cafe setting, and a young female in the living room condition.
HOW: A qualitative research was conducted in which former AUD clients experienced RECOVRY and participated in a one-hour interview afterwards. The VR experience (world selection, duration and so forth) could be viewed and controlled through laptop by the researcher and therapist or psychiatrist present at the location. To choose the order of the scenes, the researcher asked which are the most high-risk situations. The participants would always first experience the worlds without digital humans, and then with them (bar and apartment), and then experienced the other world (green world to relax). Furthermore, the two additional environments were shown to the participants after the interview. Measures: background of the recovered patients (AUD, relapses, triggers, sobriety), experience (location, triggers, craving), interaction with the virtual characters, reaction to the invitation to drink (realism and triggers), acceptance (TAM) & user intetntion and the participant’s thoughts on the virtual experience itself and design and implementation recommendations. As soon as the participant point the gaze at the avatar, the avatar moves towards the client, extends the arm and hand that holds a beverage, and offers the participant a drink through audio ("Would you like something to drink, a wine or beer or something stronger?").
WHO: The prototype was tested among 14 ex-consumers, almost all Dutch men between 50-70 years old (two women and one 33-year-old), that have undergone a long-period without alcohol (from 1 to 27 years) and of whom some work as volunteers in different facilities (Novadic-Kentron and Jellinek) to help those who are recovering.
WHERE & WHEN: at BUas (Breda) or GGD (Amsterdam) between Dec 2021 and February 2022.
RESULTS: RECOVRY was easy to control, and no participants experienced cybersickness. Adding of digital humans increased craving for most participants (for some less as they were sober for so long) and most were tempted by the invitation to drink, experiencing the offer as threatening. The adding of an avatar increased the feeling of craving in the home world, especially if the home world without avatar did not induce craving due to it not representing their own home. It did however elicit equal craving for those that drank alone when they suffered from AUD (“There is nobody... so I could have a drink without anybody knowing it.”). The invitation by the (young) women increased craving as it felt unpolite to refuse a drink offered (by the owner of the house), and due to the innocent drink invitation as she was considered to be so young (“She's not there to harm me...She doesn't have a clue probably of what she offers me.”. “She already assumes I want something with alcohol, it's hard to say no when she already has a glass of wine in her hand.”). Especially the bar scenario without people felt strange for most participants ("does not feel realistic when there are no people in") and thus the adding of avatars increased craving, even for the sneaky drinkers (alcoholic that prefers to drink alone). Reasons for not feeling craving (3 participants): the artificiality of the environment and the DHs, strong self-efficacy and motivation, the time spent without alcohol consumption. But they mentioned they would probably have felt it when they still had problems refusing alcohol. Despite that the avatars felt unrealistic and sometimes even unattractive (due to lack of emotions and expressions, limited / static movement and interaction and weird clothes and bodies), most reacted very natural and answered aloud and confirmed the avatar stimulates craving, especially due to the way they offer the drink ("The bartender is very tempting. And he doesn't even look human. This is a very strong image: he is presenting me with a bottle. I'm not ordering my drink. He's giving it to me. My brain likes that. […] He doesn't make it decide yes or no. He offers it. He doesn't make me order it. Which a good bartender does... it's difficult to say no.”). Some participants were actually anxious (but also had fun during the exposure) as they realized they accepted the alcoholic beverage in the VR. Whether the avatars could be more convincing and pushier was depended on the feelings of craving and perceived vulnerability. Almost all agreed it would stimulate craving seeing more avatars drink, the adding of emotional factors / situations and more peer pressure. Despite the limitations, the results show that digital humans constitute a valuable addition to the application: digital humans’ implementation in a VR exposure session might provide and effective solution to increase the realism of the experience in order to evoke craving in the ex-consumers. The results are consistent with the literature review and provide an explanation to those quantitative finding of the studies considered.
WHY: The feasibility study (see Study 3) revealed the desire of clients for a more realistic experience, that can be achieved by adding virtual humans to the virtual environment. Also, previous research shows ann increase in craving when digital humans are added, however that this also depends on the type of drinker, the type of interaction, the level of realism of the avatars as well as the visibility of other cues (e.g., alcohol presence). In addition, the use of CG avatars in 360 VR environments have never been studied. As such, it remains unclear what degree of visual fidelity is needed to stimulate an emotional response in simulated social interaction in the context of Cue Exposure Therapy for AUD, and how the presence of avatars affects the perceived realism of the exposure session and the craving levels of those individuals suffering from AUD. Hence, RECOVRY was updated with avatars to create social pressure by means of a virtual invitation to drink and we examined how low-fidelity avatars are experienced (level of realism) and the reasons behind how they (not) influence craving during the therapy.
WHAT: for this study RECOVRY 2.0 was developed in which we first transported and updated RECOVRY for the Oculus Quest 2 glasses (instead of Samsung VR), developed and implemented avatars in the RECOVRY 360 and CG worlds that represented the bar and the Livingroom. The avatars were avatars with a low level of realism, to reduce costs and prioritize the idea of creating many avatars and contexts (effectiveness). In addition, a call to action was created where the avatars offer a drink to the user and the user needs to select from a menu, using the Oculus Quest 2 controllers, that contains for options (a) yes, a beer, (b) yes, a wine, (c) yes, something stronger or (d) yes, but something without alcohol. This invitation to drink was offered by a male bartender in the cafe setting, and a young female in the living room condition.
HOW: A qualitative research was conducted in which former AUD clients experienced RECOVRY and participated in a one-hour interview afterwards. The VR experience (world selection, duration and so forth) could be viewed and controlled through laptop by the researcher and therapist or psychiatrist present at the location. To choose the order of the scenes, the researcher asked which are the most high-risk situations. The participants would always first experience the worlds without digital humans, and then with them (bar and apartment), and then experienced the other world (green world to relax). Furthermore, the two additional environments were shown to the participants after the interview. Measures: background of the recovered patients (AUD, relapses, triggers, sobriety), experience (location, triggers, craving), interaction with the virtual characters, reaction to the invitation to drink (realism and triggers), acceptance (TAM) & user intetntion and the participant’s thoughts on the virtual experience itself and design and implementation recommendations. As soon as the participant point the gaze at the avatar, the avatar moves towards the client, extends the arm and hand that holds a beverage, and offers the participant a drink through audio ("Would you like something to drink, a wine or beer or something stronger?").
WHO: The prototype was tested among 14 ex-consumers, almost all Dutch men between 50-70 years old (two women and one 33-year-old), that have undergone a long-period without alcohol (from 1 to 27 years) and of whom some work as volunteers in different facilities (Novadic-Kentron and Jellinek) to help those who are recovering.
WHERE & WHEN: at BUas (Breda) or GGD (Amsterdam) between Dec 2021 and February 2022.
RESULTS: RECOVRY was easy to control, and no participants experienced cybersickness. Adding of digital humans increased craving for most participants (for some less as they were sober for so long) and most were tempted by the invitation to drink, experiencing the offer as threatening. The adding of an avatar increased the feeling of craving in the home world, especially if the home world without avatar did not induce craving due to it not representing their own home. It did however elicit equal craving for those that drank alone when they suffered from AUD (“There is nobody... so I could have a drink without anybody knowing it.”). The invitation by the (young) women increased craving as it felt unpolite to refuse a drink offered (by the owner of the house), and due to the innocent drink invitation as she was considered to be so young (“She's not there to harm me...She doesn't have a clue probably of what she offers me.”. “She already assumes I want something with alcohol, it's hard to say no when she already has a glass of wine in her hand.”). Especially the bar scenario without people felt strange for most participants ("does not feel realistic when there are no people in") and thus the adding of avatars increased craving, even for the sneaky drinkers (alcoholic that prefers to drink alone). Reasons for not feeling craving (3 participants): the artificiality of the environment and the DHs, strong self-efficacy and motivation, the time spent without alcohol consumption. But they mentioned they would probably have felt it when they still had problems refusing alcohol. Despite that the avatars felt unrealistic and sometimes even unattractive (due to lack of emotions and expressions, limited / static movement and interaction and weird clothes and bodies), most reacted very natural and answered aloud and confirmed the avatar stimulates craving, especially due to the way they offer the drink ("The bartender is very tempting. And he doesn't even look human. This is a very strong image: he is presenting me with a bottle. I'm not ordering my drink. He's giving it to me. My brain likes that. […] He doesn't make it decide yes or no. He offers it. He doesn't make me order it. Which a good bartender does... it's difficult to say no.”). Some participants were actually anxious (but also had fun during the exposure) as they realized they accepted the alcoholic beverage in the VR. Whether the avatars could be more convincing and pushier was depended on the feelings of craving and perceived vulnerability. Almost all agreed it would stimulate craving seeing more avatars drink, the adding of emotional factors / situations and more peer pressure. Despite the limitations, the results show that digital humans constitute a valuable addition to the application: digital humans’ implementation in a VR exposure session might provide and effective solution to increase the realism of the experience in order to evoke craving in the ex-consumers. The results are consistent with the literature review and provide an explanation to those quantitative finding of the studies considered.
Study 4: testing 360 versus CG

WHY: test the effect of VRET (RECOVRY), and the effect of the level of realism operationalized by the type of VR (360o recording versus computer generated (CG) worlds), on craving, experience, self-efficacy and usefulness among AUD patients treated within the clinic.
WHAT: this research was based on REVOVRY 1.0 that contained no avatars. The VRET was created for SAMSUNG VR GEAR (which is paired to the Samsung Galaxy S9 smartphone), that included a router to connect the VR to a laptop in which the therapist could control and see what the patient was doing and visiting in VR (for how long). The VRET contained a safe starting zone (the clinic), three VR worlds to create craving: a bar and two home environments, for which a CG and a 360° version was created, and three safe worlds to relax: a lake, a forest and a meadow in 360° of whicht two also had a CG version (lake and meadow). The home environment consists of a clean and messy version of the apartment (in which food, bottles, glasses and ashtrays ware visible). For this study only the messy one was shown. The bar scene is a lively scene in which people are talking in the background, glasses and bottles are clinking. The CG world represents this environment as much as possible, although real persons are represented as shadow like figures. The VRET contained no interactions and were built to experience from a sitting position, where movement, except for head movement, was not possible.
HOW: Between subject design: (1) Treatment As Usual (TAU); (2) Group 360° VR Environments only (360) and (3) Group Computer Generated VR Environments only (CG). Patients received three sessions of 15 minutes of VR on day 1, 4 and 7 of their inpatient detoxification (treatment)period. The groups did not differ in age, gender, education, VR experience and knowledge (low). The non-VR group on average had more clinical treatments for detoxification before this intake and also were longer AUD patients as well felt more depended on alcohol (one of the reasons why some did not dare to take the VR treatment). Measures: questionnaires and interviews before and after the VR experiences, measuring attitude, experience (ITC-SOPI), self-efficacy (SELD-R & E), craving-vulnerability (dmCV, SSQ, heartrate, VAS), satisfaction (USEQ), accessibility, affordability, perceived ease of use, motivation and perceived usefulness (TAM).
WHO: 51 DSM-5 diagnosed AUD patients who are clinically admitted for inpatient detoxification (mean age: 46, 75% men, 95% Dutch, 61% single, 31% employed, 75% living in own house, on average 16 glasses per day over 12 years of AUD, 55% in clinic before, 80% never used VR before). Exclusion criteria: (a) Severe psychosis or hallucinations (not able to communicate), (b) Suicidal issues, (c) Severe psychiatric disorders, poly-drug use or severe physical issues (e.g., cardiovascular diseases, COPD), (d) mentally incompetent, (e) pregnancy and (f) motion sickness or balance disorders.
WHEN & WHERE: Research took place, from July till September 2019, in one of the three clinics of Novadic-Kentron in the South of the Netherlands (Breda, Eindhoven or Vught) under guidance of experienced nurses and therapists. Research was approved by the Medical Ethics Review Committee of the VU University in Amsterdam (d.d. 10-07-2019; Ref 2019-211-NL69690.029.19).
RESULTS: The VR worlds were relevant as for most the bar with friends (69%) and home (alone) worlds (77%) are craving contexts. Also, many patients attributed their own context and stories to the VR worlds and VR elements. However, for some patients the bar was not a place they usually visited to drink in real life. Moreover, some of the green worlds (like the lake or forest), caused craving as those were places some of the patients usually visit to drink. In addition, 24 patients also indicated important triggers not present, such as emotional and social related triggers (fear, fights, anxiety), visitors (friends), reward drinking (long abstinent), stress (deadlines, unexpected events), drink invitations (social), alcohol TV commercials. The VR sessions did not cause (unwanted) negative side effects for 360° nor CG condition. The worlds caused a low to moderate craving for most of the patients (for some extremely high), in an equal way between the different worlds. Some experienced more craving in 360° while others more in CG. The level of craving was higher in VR compared to control condition, was higher each time after the VR session and reduced on average over three measurements and did not differ between 360° and CG over time. In line with these results, self-efficacy increased after each session and over time (highest after three sessions: M1 = 19.7 to M3 = 22.2, scale 0-32) in both conditions (no significant differences between VR conditions). Moreover, the self-efficacy in the VR conditions was much higher compared to the control condition (the latter also did not increase over time). The physiological measurements (e.g., blood pressure) did not show strong significant differences. The participants are satisfied about the VR application (M = 3.7, five-point scale / and a 7.4 out of a 10-point scale for both GC and 360°). Main reasons for satisfaction: good for practice, helps to increase confidence, The level of satisfaction did not differ between 360 and CG condition (although 360° seemed to create a more pleasant experience). Some (four patients, two in each condition) got irritated when the VR experience did not cause craving, mainly as the worlds did not apply to them (the drink in other contexts).
Some generic improvements / suggestions: more interaction, add avatars that offer drinks, more personalization in types of drinks (as well as brands and color of bottles) and placement of drinks and food (even hide them to be discovered), ashtrays (full and empty), more worlds, better resolution, add sounds, add curtains to be closed in living room, avoid fog on lenses, glasses become too heavy or uncomfortable, missing items in CG (e.g., pool balls, doorknob), bar or living room do not represent style in their lives (but still cause craving), VRET earlier in process and on different times during the day (also in evening and weekends), half of patients would recommend using it at home as well (those who did not wanted to see either more technical improvements and/ or did not regard it as safe due to risk it would cause drinking behavior. No differences between 360 and CG were found in suggested improvements.
Conclusion: VR as an adjuvant in the treatment of AUD after clinical detoxification has been successful introduced in an inpatient setting and has yielded a number of promising results. The 360° did not outperform the CG or vice versa, which seems to ask for more research when one is preferred over the other. Further research is needed into the effectiveness in case suggested improvements are matched as well when the VR application is more used as a cue exposure therapy tool with more variation in time spend in VR (for this research it was more based on free experience).
study 3: effect of personalization
Welcome Bram Jansen
Bram was a Master of Media Innovation student at Breda University of Applied Sciences. He has chosen the Recovry project for his graduation thesis. Bram focused among others on answering the question how much the virtual worlds need to be personalized to be effective. How can we personalize VR worlds in an effective manner to help treat Alcohol Addiction, and how will this help to create a more effective VRET application? Moreover, if organizations choose to personalize VRET environments, which elements are the most important to personalize and as such elicit a stronger feeling of craving for Alcohol-use Disorder patients? Not much is known about person-specific cues that create unique experiences to increase craving.
Previous studies, however, identified a range of elements capable of eliciting craving in AUD-patients. These are cues that have been examined in studies before: presence of alcohol (sounds of glasses in bars, seeing different alcoholic drinks, seeing and smelling others hold or drink alcohol and alcohol-related words), emotional factors (negative and positive), social factors (peer pressure), time factors (time of the day and day of the week), (social) environments (Pubs, Restaurants, Bars, Parties, Within the house, Parks and other public spaces, During meals and Kitchens). For instance, night and afternoon created more craving compared to midday or morning, and weekends are more difficult to resist drinking. Being with peers and social pressure increased craving and alcohol intakes. However, high levels of craving are also high when being alone or with friends instead of being with relatives, partner or co-workers. Positive and negative emotions also elicited craving, although negative emotions generally show greater self-reported craving. Parties, restaurants, bars, pubs, being at home and being in a club elicited the highest levels of craving, whereas the living room, the kitchen, the workplace, the bedroom, the supermarket or being in parks showed craving, but less.
Time to so dome investigation by ourselves.
Participants: 10 DSM-V diagnosed AUD-patients (between 18 and 65 years old) during the last week of their inpatient detoxification at one of the Novadic-Kentron detoxification units at Breda, Vught, or Eindhoven. Patients who experienced severe psychosis, hallucinations, suicidal issues, severe psychiatric disorders, severe poly-drug use that impeded treatment, or severe physical issues such as cardiovascular diseases were excluded from the study due to health risks or potentially skewed results. A pre-study (by Reimink) showed the success of the manipulation: the clinic’s entrance hall was indicated as a neutral place, a bar and a home situation were indicated as risk scenes, the natural surrounding with trees was indicated as a safe zone.
Design: The participants experienced Recovry 1.0 on the Samsung Gear VR and Samsung Galaxy S9. The scene selection and duration were in the hands of a therapist. All sessions followed a similar pattern: (a) introduction, (b) 'before exposure' questionnaires, (c) heart rate and blood pressure measurements, (d) VR experience (three sessions using graded exposure and each time ending with 'relaxation' environment), (e) post experience heart rate and blood pressure measurements, and (f) 'after exposure' questionnaires and the final session also included an (g) interview.
Negative Results: due to the design, craving in general was low. The therapy and detox already increased self-efficacy and motivation, and some participants even had visited bars without drinking during a leave of absence This reduced the impact of virtual exposure. The CG bar scene lacked social cues for some, due the unsociable (boring) context (no people visible, abstract design such as shadow figures and poor furnished, although the pool table did create craving), the visibility of the alcohol was low (e.g., only few bottles behind the bar and being too abstract) and no peer pressure (like an invitation to drink). Finally, the technical execution can have a negative impact: the 360 resolution was not optimal and as such could break the feeling of presence.
Positive results: However, within the CG and 360 worlds, the craving was mainly stimulated through the apartment scene and primarily by the presence of alcohol (visual cues such as ashtrays beer bottles, cigarettes, beer cans and bottles of wine), and social cues (the left-open fridge, the couch and food as a general reminder of a party the night before), which were perceived as relaxed drinking with others.
Personalization needed: The study showed that the craving elicited by the type of environment is dependent on the individual’s past experiences. Not only the choice of environment is important, also the way the alcohol is present in the environment needs to be personalized. For some the mess in the apartment worked, for some it did not as they were used to hide their drinking at home. For some the bar was cosy and social, for others the bar was boring and outdated and did not represent “their bar”. The same goes for the visibility of alcohol: generic bottles were often confusing for participants, they either needed wine or beer bottles, depending on their drinking preference. The style, 360 or CG, seems to be a matter of personalization as well: some preferred CG, some preferred 360.
The conclusion seems obvious: some level of personalization is needed on all craving dimensions. First, there is no clear preference for 360 or CG. Both work for different people. Seconds, the environments are depended on personal history and associations they need to represent different levels of alcohol visibility (messy or clean), and types of drink (based on past drinking behavior), and different emotional contexts are needed (positive and negative). In addition, for reasons of protection (medical research) the craving was deliberately kept low. However, when a VRET needs to reach people after detox and therapy, despite grading exposure, the starting craving level needs to be higher.
Bram was a Master of Media Innovation student at Breda University of Applied Sciences. He has chosen the Recovry project for his graduation thesis. Bram focused among others on answering the question how much the virtual worlds need to be personalized to be effective. How can we personalize VR worlds in an effective manner to help treat Alcohol Addiction, and how will this help to create a more effective VRET application? Moreover, if organizations choose to personalize VRET environments, which elements are the most important to personalize and as such elicit a stronger feeling of craving for Alcohol-use Disorder patients? Not much is known about person-specific cues that create unique experiences to increase craving.
Previous studies, however, identified a range of elements capable of eliciting craving in AUD-patients. These are cues that have been examined in studies before: presence of alcohol (sounds of glasses in bars, seeing different alcoholic drinks, seeing and smelling others hold or drink alcohol and alcohol-related words), emotional factors (negative and positive), social factors (peer pressure), time factors (time of the day and day of the week), (social) environments (Pubs, Restaurants, Bars, Parties, Within the house, Parks and other public spaces, During meals and Kitchens). For instance, night and afternoon created more craving compared to midday or morning, and weekends are more difficult to resist drinking. Being with peers and social pressure increased craving and alcohol intakes. However, high levels of craving are also high when being alone or with friends instead of being with relatives, partner or co-workers. Positive and negative emotions also elicited craving, although negative emotions generally show greater self-reported craving. Parties, restaurants, bars, pubs, being at home and being in a club elicited the highest levels of craving, whereas the living room, the kitchen, the workplace, the bedroom, the supermarket or being in parks showed craving, but less.
Time to so dome investigation by ourselves.
Participants: 10 DSM-V diagnosed AUD-patients (between 18 and 65 years old) during the last week of their inpatient detoxification at one of the Novadic-Kentron detoxification units at Breda, Vught, or Eindhoven. Patients who experienced severe psychosis, hallucinations, suicidal issues, severe psychiatric disorders, severe poly-drug use that impeded treatment, or severe physical issues such as cardiovascular diseases were excluded from the study due to health risks or potentially skewed results. A pre-study (by Reimink) showed the success of the manipulation: the clinic’s entrance hall was indicated as a neutral place, a bar and a home situation were indicated as risk scenes, the natural surrounding with trees was indicated as a safe zone.
Design: The participants experienced Recovry 1.0 on the Samsung Gear VR and Samsung Galaxy S9. The scene selection and duration were in the hands of a therapist. All sessions followed a similar pattern: (a) introduction, (b) 'before exposure' questionnaires, (c) heart rate and blood pressure measurements, (d) VR experience (three sessions using graded exposure and each time ending with 'relaxation' environment), (e) post experience heart rate and blood pressure measurements, and (f) 'after exposure' questionnaires and the final session also included an (g) interview.
Negative Results: due to the design, craving in general was low. The therapy and detox already increased self-efficacy and motivation, and some participants even had visited bars without drinking during a leave of absence This reduced the impact of virtual exposure. The CG bar scene lacked social cues for some, due the unsociable (boring) context (no people visible, abstract design such as shadow figures and poor furnished, although the pool table did create craving), the visibility of the alcohol was low (e.g., only few bottles behind the bar and being too abstract) and no peer pressure (like an invitation to drink). Finally, the technical execution can have a negative impact: the 360 resolution was not optimal and as such could break the feeling of presence.
Positive results: However, within the CG and 360 worlds, the craving was mainly stimulated through the apartment scene and primarily by the presence of alcohol (visual cues such as ashtrays beer bottles, cigarettes, beer cans and bottles of wine), and social cues (the left-open fridge, the couch and food as a general reminder of a party the night before), which were perceived as relaxed drinking with others.
Personalization needed: The study showed that the craving elicited by the type of environment is dependent on the individual’s past experiences. Not only the choice of environment is important, also the way the alcohol is present in the environment needs to be personalized. For some the mess in the apartment worked, for some it did not as they were used to hide their drinking at home. For some the bar was cosy and social, for others the bar was boring and outdated and did not represent “their bar”. The same goes for the visibility of alcohol: generic bottles were often confusing for participants, they either needed wine or beer bottles, depending on their drinking preference. The style, 360 or CG, seems to be a matter of personalization as well: some preferred CG, some preferred 360.
The conclusion seems obvious: some level of personalization is needed on all craving dimensions. First, there is no clear preference for 360 or CG. Both work for different people. Seconds, the environments are depended on personal history and associations they need to represent different levels of alcohol visibility (messy or clean), and types of drink (based on past drinking behavior), and different emotional contexts are needed (positive and negative). In addition, for reasons of protection (medical research) the craving was deliberately kept low. However, when a VRET needs to reach people after detox and therapy, despite grading exposure, the starting craving level needs to be higher.
Study 2: VR concept testing

Klara finished her graduation with a very good study, showing the potential of the Recovry Application. The VR prototype was tested through interviews among 14 users divided over (former) AUD clients, psychologists, and nurses. The results indicated that both 360 and cg created VR worlds, helped patients with their treatment. The VR seems to trigger feelings of craving: “The apartment version was quite confronting....yeah, I saw myself sitting on the couch and drinking. That came to my mind. And the bar scene was a little trigger ....." . The most clear factor seems to be hedonic. The VR application was experienced as engaging without drawbacks that helped to stimulate going through therapy: “I think that in the beginning it's the entertainment and then you have a thing to talk about...it's great because a lot of the clients [otherwise] don't see the triggers. ....it's easier because these environments are normally not inside of the clinic ..". It seems that participants prefer the 360° version over the computer-generated (CG) one because it felt more real and induced more presence: "The real films, the real pictures are the ones that do it for me, not the computerized ones". In addition the study showed that a graded exposure treatment is recommended. Meaning that it should start with a less immersive CG experience before going into the 360 recorded worlds: Yes if they want the experience and to practice I think the realistic one is more useful. But if in the computer one are details I think it's the first step maybe to practice...in steps, so you begin with easy and you and then you build up to the realistic one, to the filmed one". In addition personalization of the worlds might work more effective, although clients also were not sure whether that might be to confrontational, preferring a graded exposure as well when it comes to personalization: “Maybe in the first place practice not in the own situation....after having practiced more try your own surrounding". The study provided many more recommendations on design, content and usage. But most important, it provided enough promising results to go forwards with the effect study. Thank you Clara for your important contribution!
Study 1: discovering risk environments to build in VR
Together with Utrecht University (Anne Reimink), we conducted our first study aimed at discovering environments (contexts) that create alcohol craving and that can efficiently be recreated inside VR (CG and 360) in order to develop RECOVRY 1.0.
WHY: Craving is described as a strong appetite, desire or urge to drink alcohol. Therefore, addiction treatment is primarily focused on reduction of craving (conditioned responses) or on dealing with how to cope with craving through means of self-efficacy and coping skills (and thus reduce relapse). In case of AUD, self-efficacy means the belief to be able to stay abstinent of alcohol consumption in high-risk situations and cues (contexts) that trigger craving for alcohol consumption. These contexts and cues are present in in everyday life in all kinds of (social) situations, which makes exposure to alcohol-related cues impossible to avoid. Cue exposure therapy (CET) is based on treatment through repeated exposure to these environments. Virtual Reality Exposure Therapy (VRET) provides the possibility to train in safe, real-life personalized situations that feel real using more cues and contexts at the same time compared to other CET treatments. However, to develop such a tool, it needs to be clear what environments need and can be developed that apply for many (former) AUD clients.
Therefore, the goal of this research was to assess which environments and cues could be experienced as high-risk situations for relapse (that are most likely to elicit craving on the one hand but on the other hand can be successfully and efficiently be implemented in VR to increase coping-skills and self-efficacy). These environments then would receive priority to be developed as VR worlds to be used in a new VRET tool (RECOVRY).
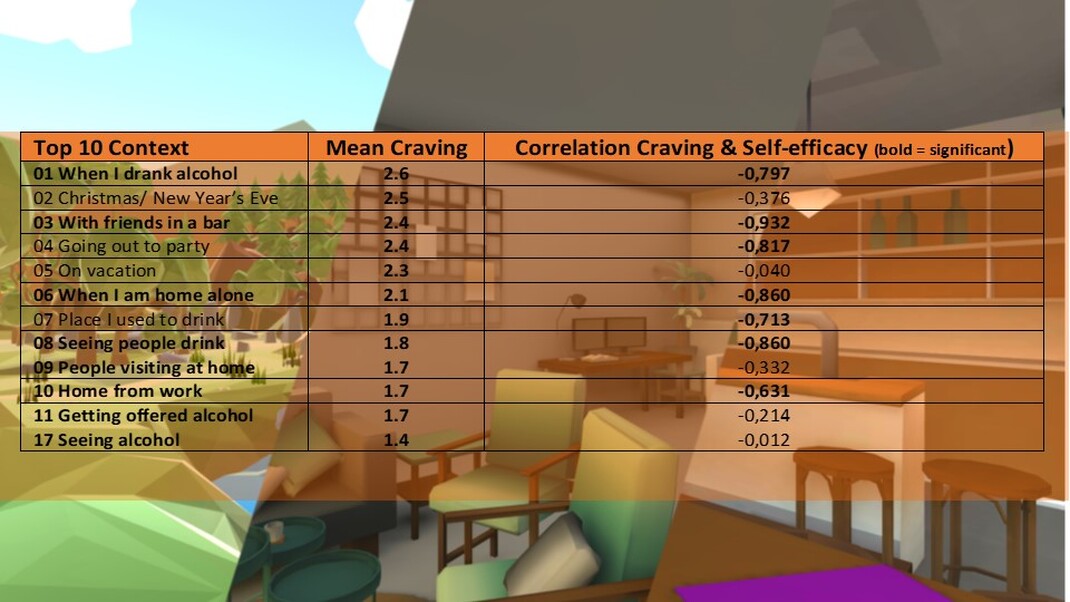
HOW: (a) descriptive research: analyze high-risk situations that are used in AUD related CET and (b) qualitative research: interviewing AUD inpatients in which they had to rate the level of craving (0 = no craving, 4 = very strong craving) and self-efficacy (0 = no self-efficacy, 5 = very much self-efficacy), and level of perceived risk (1 = low, 2= high) for relapse for 31 high-risk environments based on a workbook used in cognitive-behavioral therapy. The focus was on physical surroundings as a first step to build in VR and less on emotional contexts (as these are more complex and expensive to create).
WHO: 13 alcohol dependent inpatients (adults with an average age 50 and 75% male), were interviewed with a primary diagnosis of alcohol dependence and fulfilled the diagnostic criteria for alcohol dependency according to DSM-V (on average 18 years of use before first treatment), had been in detoxification treatment for at least 4 days (average of ten days), with abstinence from psychoactive recreational drugs during treatment and no severe psychiatric or intellectual disability or impairment. All participants were depended on another drug as well (often nicotine and THC or Cocaine), and almost half had justice issues.
WHAT: alcohol-dependent inpatients can clearly differentiate which environmental cues form a trigger for their relapse. A challenge to create an efficient VRET related to AUD is the diversity of worlds and situations that trigger craving. Based on the self-reported levels of craving and self-efficacy two environments were selected out of the top ten perceived high-risk situations: (1) Being in a bar (seeing alcohol) and (2) Being at home (alone and seeing alcohol). Both environments we combined (in RECOVRY 2.0) with three top ten risk contexts: (a) when I drank alcohol, (b) seeing people drink and (c) getting offered alcohol.